Invalid Link Removed lechatroom.com/forum/showpost.php?p=40976&postcount=5
Actually, I don't think there is much difference between the two (extract vs recombinant) at least not enough to worry about. Here is a study that has it the other way around JanSz.
"Recombinant hCG at a dose of 250 mg (6500 IU) gives the same results as 5000 IU extractive hCG."
Evaluation of endocrine testing of Leydig cell function using
extractive and recombinant human chorionic gonadotropin and
different doses of recombinant human LH in normal men
From: European Journal of Endocrinology (2008) 159 171–178
(6500iu)rHCG=(5000iu)HCG
------------
Invalid Link Removed
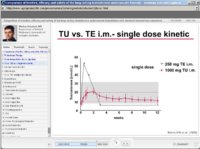
Results: ehCG induced dose-dependent increases in plasma estradiol and testosterone levels. They respectively peaked at 24 and 72 h after the injection. The most potent dose of ehCG (5000 IU) induced results similar to those observed with 250 µg (6500 IU) rhCG. By comparison with placebo, rhLH induced a significant and dose-dependent increase in plasma testosterone levels 4 h after the injection. Peak response of testosterone to rhLH and rhCG was significantly correlated. rhLH did not induce significant change in plasma estradiol level.
Conclusions: In normal men, a single i.v. injection of 150 IU rhLH induces a 25% rise in plasma testosterone levels by comparison with placebo. At the moment, the dynamic evaluation using hCG remains the gold standard test to explore the Leydig cell function. The use of 250 µg rhCG avoiding any contamination should be recommended.
====================================================================
Invalid Link Removed
HOW SUPPLIED
Ovidrel® PreFilled Syringe (choriogonadotropin alfa injection) is
supplied in a sterile, liquid single dose pre-filled 1 mL syringe. Each
Ovidrel® PreFilled Syringe is fi lled with 0.515 mL containing 257.5
μg of chorio-gonadotropin alfa, 28.1 mg mannitol, 505 μg 85%
O-phosphoric acid, 103 μg L-methionine, 51.5 μg Poloxamer 188,
Sodium Hydroxide (for pH adjustment), and Water for Injection to
deliver 250 μg of chorio-gonadotropin alfa in 0.5 mL.
The following package combination is available:
• 1 pre-filled syringe containing 250 μg Ovidrel® PreFilled Syringe
NDC 44087-1150-1
====================================================================
Mixing instructions.
250 µg rhCG =(6500iu)rHCG=(5000iu)HCG=0.515 mL=51.5units(on insuline syringe)
Lets make solution having total volume=2.5 mL=250units
Lets use units of "regular/natural" HCG
That solution will have density of
(5000iu)/(2.5mL)=2000iu/mL=(2000iu)/(100units)=20iu/unit
To empty sterile vial add
content of Ovidrel syringe=0.515mL
and
2.5mL - 0.515mL=~2mL bacteriostatic water
250iu =250/20=12.5units
300iu =300/20=15units
400iu =400/20=20units
500iu =500/20=25units
600iu =600/20=30units
all above can be handled by the smallest syringe:
BD Ultrafine II U-100 Insulin Syringe 31 Gauge 3/10cc 5/16inch Short Needle--1/2 Unit Markings
===================================================================
Invalid Link Removed lechatroom.com/forum/showpost.php?p=48255&postcount=11
July/31/2009
I mix my 0.5 mL (250 mcg) Ovidrel with 2.5 mL water.
Each day I inject 0.08 mL (6.7 mcg) of the combined mixture. It lasts around 37 days.
Plus I also apply a little transdermal T (testosterone) gel / cream daily.
I get most of my T boost from HCG, but not all. Like Dr Crisler, I also believe that we do need daily variability in our T levels.
===========================================================
Invalid Link Removed lthingsmale.com/pdfs/instructions/USE_OVIDREL.pdf
Ovidrel mixing instructions from Dr. John's forum.
You need the Ovidrel injection, which is a .5ml injection equivalent to
10000iu of HCG. You need bacteriostatic water and a sterile vial.
Draw out 9.5 ml of the BC water and inject into the sterile vial. Inject the
Ovidrel into the sterile vial with the 9.5ml BC water and mix GENTLY to end
up with a total of 10 ml. Then 25 units on an insulin syringe will be the
equivalent of 250iu of HCG. This will last 20 weeks at the 250iu 2x a week
dosing. Prescribe one injection at a time, potency lasts longer.
BD Ultrafine II U-100 Insulin Syringe 31 Gauge 3/10cc 5/16inch Short
Needle--1/2 Unit Markings
The advice for script is to simply say "use as directed".
-------------
Invalid Link Removed
Ovitrelle 250 mcg Serono Syringes $79.00
Generic Name: Choriogonadotropin Alfa
In order to buy Ovidrel online you will require a valid prescription
===================
===================
Invalid Link Removed
Ovitrelle syringe 250mcg
=================
=================
Invalid Link Removed lechatroom.com/forum/showthread.php?14401-Clomid-instead-of-HCG&p=144967#post144967
That's only because your HCG dose was too low.
The response to HCG varies very widely amongst males.
You and your medical professional adviser know your HCG does is close to optimum when your testicle size is restored back to where they were before you started supplementing with exogenous T. The concept of a fixed dose of HCG (eg: 500IU) being optimal is not reliable, and has definitely not been validated among a wide sample of males.
eg: in order for my testicle size to be close to where they were before I started hormone modulation therapy, I have to supplement with around 34 micrograms of HCG (as ovidrel) per day, which amounts to either:
a) 800 IU per day (if you believe 250 mcg of Ovidrel HCG = 6,000 IU urinary derived HCG)
or:
b) 1350 IU per day (if you believe 250 mcg of Ovidrel HCG = 10,000 IU urinary derived HCG).
I am a well known hypermetabolizer of testosterone, but that's not relevant to testicular size, because most of our testicular size is due to sertoli cells, which are triggered by FSH. Ie: only a much smaller fraction of our testicular size is due to the leydig cells which are tirggered by LH in order to make testosterone.
.
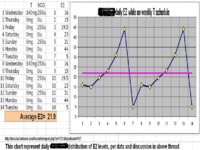
There is research paper correlating HCG dose with 17-hydroxy-progesterone (healty individuals tested)
do you
accept those findings
measure your 17-hydroxy-progesterone
Other than testicle size
what would you miss in significant way, if you reverted to 350iu/EOD (as supported by above research?
=============================
5/14/2011
Invalid Link Removed clechatroom.com/forum/showthread.php?17926-HCG-amp-Ovidrel-protocol&p=145668#post145668
Re: HCG & Ovidrel protocol
Originally Posted by JanSz
There is research paper correlating HCG dose with 17-hydroxy-progesterone (healty individuals tested)
They obviously didn't encounter any hypermetabolizer males amongst their group.
Hypermetabolizers need far more HCG than "average" in order to stay optimum.
Originally Posted by JanSz
Other than testicle size
what would you miss in significant way, if you reverted to 350iu/EOD (as supported by above research)?
35mcg of Ovidrel per day (900 IU per day) is for me a baseline minimum. I take 17 mcg (450 IU) at 7am, and 17 mcg (450 IU) at 7pm.
Some days I need to increase HCG dose above 35mcg (900 IU) per day because I've been extra energetic during the week. I always notice the symptoms of too low T around the middle of the day. On such days I have to increase my 7pm dose of HCG to be even greater than 17 mcg (450 IU) to compensate. My medical professional adviser allows me to adjust my dosage in this way.
=================================================
=================================================
Invalid Link Removed clechatroom.com/forum/showthread.php?17988-Help-Ups-and-Down-of-HCG-amp-TRT&p=147133#post147133
Actually I now apply 800 IU of HCG daily, every day.
I had to switch to 800 IU daily PLUS 1.6 grams of testosterone applied transdermally daily.
I had to make this switch once my thyroid hormone levels increased to youthful, because I increased the rate I excrete testosterone, and I was finding that on "transdermal-only" days it was too messy trying to apply 3.2 grams of testosterone applied transdermally, as 16mL of 20% testosterone. (JanSz comment, this must be typo, 1.6mL)
As it is, my body completely absorbs 4mL of testosterone in lipoderm within 12 hours, so when I apply my second dose of transdermal T around 12 hours after my first dose, then the original area is almost completely dry.
Note that before I started boosting my resting metabolic rate, my skin was still a little grasy 24 hours later, on the few occasions when I had to apply large doses of T (eg: when I was ill).
In other words, absorption is entirely dependent on resting metabolic rate.
.
My own benchmark when using TD testosterone, 10grams/day Androgel(1%)-->100mg/day testosterone
TT=1100, SHBG~18, BAT~575, Albumin=4.3
no HCG at that time, completely shrunken testicles
---------------------------------------------------------------------------------------
Assume 1gram=1mL (often it is closer to 1mL=0.9gram)
1.6grams of 20% TD testosterone contains 1.6*1000*0.2=320mg testosterone
This are huge amounts of testosterone.
I am concerned that lots of test does not enter the system.
It would help me in understanding if you could post TotalTest in serum on such a protocol.
If that is not asking for too much, please
TT, SHBG, Albumin
For privacy, PM would be ok too.
===============================================
I would appreciate if you could discuss thyroid hormones numerically.
I am still working on assumption that for 99% of us TSH provides resonable indication.
That is, while supplementing with any combination of T4 and or T3, from pov of TSH the goal is
TSH(0.5-1)
As it is, my body completely absorbs 4mL of testosterone in lipoderm within 12 hours, so when I apply my second dose of transdermal T around 12 hours after my first dose, then the original area is almost completely dry.
Note that before I started boosting my resting metabolic rate, my skin was still a little grasy 24 hours later, on the few occasions when I had to apply large doses of T (eg: when I was ill).
Where are you applying testosterone? I am concerned, if skin stays moist for almost 12 hrs (or sometimes 24hrs), it must be exposed skin (face, neck) otherwise most of it will rub off clothes.