Well, I couldn't begin to comment on what you see in your practice and how you treat patients, but I appreciate you sharing that info here Dr. John.
I guess what I took from this thread was a couple of different points with regards to the progestin gyno issue. I think one of the things that LG was trying to say early in the thread is that on this and other boards you can find lots of references to such and such steroid/prosteroid/prohormone being a "progestin" and thus a string of warnings for people to watch out for gyno (which isn't a bad warning under any circumstances, really). However, many of these compounds, at least from what I can tell, are not, in fact progestins, at least in a strictly chemical sense. Here's Pat Arnold talking about progestins:
"most of these componunds people are calling progestins are not really progestins. they share vague chemical similarity with known pharmaceutical progestins and maybe have slight progestational activity but in my expert opinion would NOT fall into the category of progestin. they would be considered in the androgen class.
case in point would be estra-4,9-dien-3,17-dione
-------------
[a] progestin is something that has progestational activity. but the complicated thing is most androgens have a certain degree of progestational activity (albeit minor for most)
its really a subjective call. certainly something like norethindrone from birth control pills can be considered a progestin (even though it has substantial androgenic activity). and then norethandrolone would be considered an androgen (even though it is very close in structure to norethindrone and has substantial progestational activity)
then there is the chemical aspect of what is a progestin
there are two classes of progestins - the C20-keto progestins such as classic progesterone and its derivatives, and the 17alpha-ethynyl estren derivatives such as norethindrone and norgestrel
i would think anything that is not in these structural classes would not be considered a progestin by an authority in this field. the only supplement i am aware of that fit this definition was the stuff that was in the old methyl-1-p (which was a C20-keto derivative)"
So the problem, to me, is that while most of these compounds cannot be chemically classified as progestins, it is, as PA said, possible that some of them (or some of their metabolites) may have some level of activity at the progesterone receptor. I, for one, would like to see such info for many of these compounds, but I doubt that I could scour PubMed for the next year and be able to compile a halfway decent chart of "compounds and their metabolites that may or may not have progestational activity (that may or may not lead to gyno)"
Anyway....see if this makes sense
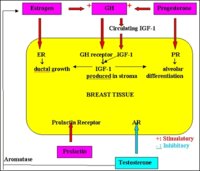
Progestin/progesterone ---> increased progesterone receptor signaling (which leads to)
--> increased IGF-1 expression
----> stimulation of alveolar hyperplasia (does this contribute to gyno?)
--> lowered DHT levels
-----> decreased antiestrogenic DHT activity in breast tissue
-----> decreased DHT block of estrogen receptors in breast
-----> decreased DHT anti-aromatase activity in breast
? where does prolactin come into this? It seems like it is the combined rise in estrogen and progesterone that contributes, i.e. progesterone causes development of the gland, and estrogen causes accumulation of prolactin that will eventually cause secretions...
In women, the drop in estrogen and progesterone after birth basically releases a hold on prolactin induced secretion...what is the equivalent process in men?
A second question for you Dr. John, or anyone really, is why is deca (nandrolone) considered a progestin, as chemically it doesn't fall into either of the classes PA describes above? Is this simply because it is known to act on the progesterone receptor despite being an androgen (in the literature)? If so, I think one source of confusion in these discussions across the various boards is that activity (progestational) trumps structure. To me, it would be better to say deca is an androgen with high progestational activity than calling it a progestin (but that's just me...I don't know how it is looked at in the field of endocrinology).
As far as DHT vs. progesterone for treatment of gyno...is it possible that there is sort of a dose-response to progesterone that might be beneficial, i.e. a low dose that might do what LG says and serve to add an additional layer of protection (added to your SERM tx) by downregulating estrogen receptor expression, whereas higher doses would actually be much worse b/c it would induce the changes listed above? (just trying to square the two sides of the debate, which may not be possible...though I don't think the two sides were that far before it got a little heated...in one of LGs early posts he does argue that low DHT may be a primary aggravator of gyno).
Anyway...sorry for the rambling...just trying to throw some more talking points out there. Let me know if I'm making sense or way off track...