TheBGRigatoni
Well-known member
- Awards
- 1
Thanks for the followLooking forward to seeing if we have a winner here!

Thanks for the followLooking forward to seeing if we have a winner here!
This is why i'm hesistant to pull the trigger. I'm living on a budget these days, so I'd prefer to buy something that actually works.yea, the amount per serving is what has me like :/ uhhh.... but it is a bold step, so hopefully it works.
...don't have the bottle pic pulled up...is that 120 caps per bottle...so a bottle lasts 20 days?It's actually correct. 3 caps is a total of 30mgs ultra 1-DHEA. We believe our hormone shield is superior to the point that a larger dose is not necessary, nor is it financially feasible for your typical guy.
It's a 28 day supply, or 168 caps IIRC....don't have the bottle pic pulled up...is that 120 caps per bottle...so a bottle lasts 20 days?
We actually believe it's quite a bit higher than we ever initially though it would be. The sublingual studies hinted at that, but then the AMS 1-Androsterone urinary excretion study (third party) supported it even further. That showed us it appeared to convert to the diol, and testosterone quite efficiently. The problem with the old stuff and the new stuff is the delivery. The bioavailability of a typical capsule of un-esterfied 19-norDIOL is less than 1%. That is why you had guys dosing it as high as a gram. But sublingual 19-norDiol had an estimated bioavailability closer to 68%. Which is why such a little dose had such a nice biological effect. I'm using 19-norDIOL in this example just because there is good research behind it. Sublinguals have some limitations though.What type of conversion rate to 1-T are you guys projecting with this?
1-T supps back in the day were dosed at what? 100-300mg? 1-AD (original) was dosed in the 200-400 and was a one step conversion to 1-T? This is a 2 step starting at 30mg...you guys must be loving this hormone sheild complex.

thanks bud good postWe actually believe it's quite a bit higher than we ever initially though it would be. The sublingual studies hinted at that, but then the AMS 1-Androsterone urinary excretion study (third party) supported it even further. That showed us it appeared to convert to the diol, and testosterone quite efficiently. The problem with the old stuff and the new stuff is the delivery. The bioavailability of a typical capsule of un-esterfied 19-norDIOL is less than 1%. That is why you had guys dosing it as high as a gram. But sublingual 19-norDiol had an estimated bioavailability closer to 68%. Which is why such a little dose had such a nice biological effect. I'm using 19-norDIOL in this example just because there is good research behind it. Sublinguals have some limitations though.
We are working on an article that compares oral vs. sublingual vs. this delivery method and outlining our estimates for bioavailability for each. We are still discussing where it falls and how we want to advertise that exactly but it's coming. As you can probably guess though this system is superior to both. Although without the Hormone Shield I dont think it would be as good as the sublinguals.
Just as an example, that study I referenced above that was brand new on berberine showed it increased the bioavailability of the drug tested 38-40%. That's very significant.
As a straight up estimate (there is no pharmacokinetic research on this stuff so it is just an estimate) it is somewhere like this:
1 sublingual tab = 200-300mg's of an oral capsule
1 dose of Alpha Mass = 300-500mg's of an oral capsule
Note: I may change my thoughts on this depending upon on the logs go bros. I think it might have an even greater potential.
Yeah, just say it's awesome and it works because I say so. That's what we want to hear/believe.My boss tells me I'm too long winded.
That's true to some point. As your test levels increase the body will likely down regulate the androgenic producing peripheral enzymes as a response. This is probably the reason prohormones tend to work better in older guys (lower test levels thus upregulating of critical peripheral enzymes.With all the various dosages and delivery systems for higher bio-availability, it left me wondering if there is a saturation point where more will not be necessary.
That actually works for the bros in the supp shops and gyms to some degree. Not so much the board crew as you know.Yeah, just say it's awesome and it works because I say so. That's what we want to hear/believe.
I think a better cycle will be five weeks or less at a higher dose as opposed to a long low dose cycle.so you wouldnt suggest an 8 week cycle?
Just from what I have read this is how I visualized the process.So, maybe something like a 7-8 week Legal SARM run finished with 4-5 week Alpha Mass for 12 weeks total?I think a better cycle will be five weeks or less at a higher dose as opposed to a long low dose cycle.
You have the right idea. Or even 4-5 weeks with prohormones followed by a methyl for 3-4 weeks. That's assuming the methyl is an active steroid, which basically eliminates the peripheral enzymes needed for the conversions.So, maybe something like a 7-8 week Legal SARM run finished with 4-5 week Alpha Mass for 12 weeks total?
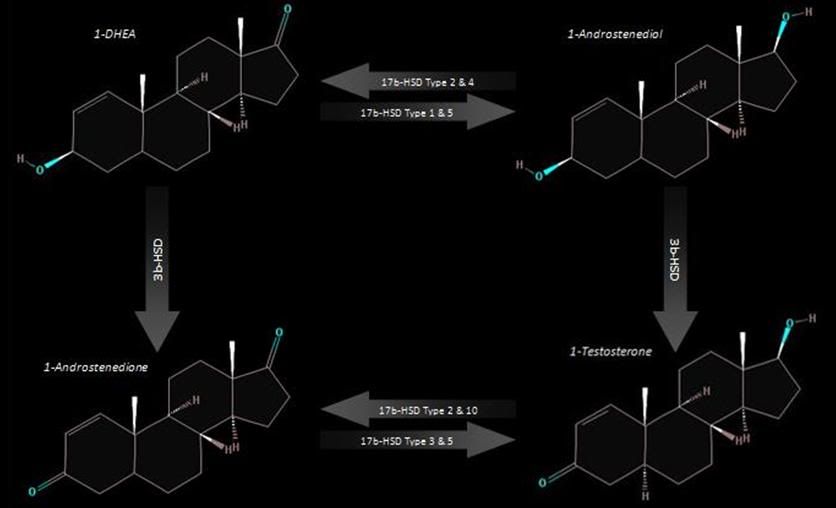
They do compete for the same enzymes. This illustrates the conversion pathways of 1-DHEA, but you could plug in 4-DHEA, 19-norDHEA, and even a few other prohormones at the same spot as 1-DHEA and follow either path. So really in situation 1 or 2 it wont vary. The difference you may see is some synergy between compounds. Example 1-DHEA and 4-DHEA will be popular simply because it will be relatively side effect free, but it wont create as good of gains as 1-DHEA alone at an equivalent dose, or even 1-DHEA + 19-norDHEA. Does this answer your question? Or at least help?Hmm.. I have all kinds of questions now. If you don't mind me asking, since there are 2 approaches you mentioned e.g. do not exceed 5 weeks at recommended, and\or a higher dosage at 5 weeks or less.
I want to throw in a variable here of another ph for example when stacking AlphaMass with lets say a 4-dhea compound. Regardless if it is a higher dosage or recommended dosage, is there the possibility of competing pathways, or is there a way to actually mitigate that, and can that happen if you take a larger dose on a 4-5 week cycle for a single compound.
I'm looking at 2 scenarios:
1. A stack where compounds compete for the same pathway, causing one not to get the desired results (diet and hard work are assumed to be in place)
2. A single compound at a higher dose causing a saturation point, or just to much for the pathway to absorb.
If the wording sounded dumb, it's cause I'm not a scientist or bio-chemist major, minor or anything
Makes sense based on some of the research. I think this is also why you see more variability when it comes to gains when dealing with PH's vs. something like superdrol. Still it's about 19,000 times easier on the system.i've noticed that when running pro hormones. low dosages start out good, but i keep having to increase the dosage to get the same effect. it's how i ended up at 1,000mg of 4-ad.
It does help and am doing some reading on neurochemistry as a result to gain a better understanding. I mean for all intents and purposes we are dealing with activation via 3b-hsd and 17b hsd type 2 & 10 into 1-testosterone. However it seems that this can bounce back and forth e.g. activation and deactivation.They do compete for the same enzymes. This illustrates the conversion pathways of 1-DHEA, but you could plug in 4-DHEA, 19-norDHEA, and even a few other prohormones at the same spot as 1-DHEA and follow either path. So really in situation 1 or 2 it wont vary. The difference you may see is some synergy between compounds. Example 1-DHEA and 4-DHEA will be popular simply because it will be relatively side effect free, but it wont create as good of gains as 1-DHEA alone at an equivalent dose, or even 1-DHEA + 19-norDHEA. Does this answer your question? Or at least help?
I think you are looking at the arrows incorrectly. Type 2 and 10 actually convert the hormones back into less powerful prohormones. But you do have the right idea that the conversions are not 'static' and they can be moving back and forth depending upon the tissue it interacts with...It does help and am doing some reading on neurochemistry as a result to gain a better understanding. I mean for all intents and purposes we are dealing with activation via 3b-hsd and 17b hsd type 2 & 10 into 1-testosterone. However it seems that this can bounce back and forth e.g. activation and deactivation.
So I think a bit sunk in the memory bank
Now, what about synergy? I got incomplete info which did not go into details or nothing actually and just said that by stacking you get the effect of 1+1=3 or if you add more 1+1+1=5, and did not explain what prohormones are synergistic.
Also on that note, I don't think you necessarily need to stack phs with phs, but instead you can enhance the effect using certain supplements such as creatine, l-carnitine-l-tartrate, DAA (read somewhere its good to do throughout a cycle for easier recovery).
I appreciate the information and education you are giving, it's actually really cool.
Thanks!
I wish I could easily answer that, and it's something to look into for sure. However, after a lay off just like your hormonal system these enzymes will recover. So assuming you take adequate time off you should be fine.A quick question comes to mind though. I've been planning on a run with the alpha mass product and the deca sarm product from ams. My question is after a nice long 12 week cycle of deca sarm and then a pct would it not be a good idea to run a ph like alpha mass but instead something that was active on it's own like epi so as to give the enzymes enough time to re up so to speak.
LOL! Yes I definitely didI think you are looking at the arrows incorrectly. Type 2 and 10 actually convert the hormones back into less powerful prohormones. But you do have the right idea that the conversions are not 'static' and they can be moving back and forth depending upon the tissue it interacts with...
Synergy was a bad word. I should have said "complimentary". Think of it like this:
Gains in size/strength - on a scale of 1-10 with 10 equaling great gains
12 caps of Alpha Mass/day = 10
6 caps of Alpha Mass + 6 caps of Alpha Bulk (4-DHEA product) = 5-8
Side effects (ex. lethargy, libido loss) - on a scale of 1-10 with 10 equaling bad sides
12 caps of Alpha Mass/day = 10
6 caps of Alpha Mass + 6 caps of Alpha Bulk (4-DHEA product) = 4-6
Or something similar to the above.
The formula you provided makes sense if one is willing to forgo the sides, or go with a conservative approach. This gives me lots to think about and consider. Will let AM minds know..right now Alpha Mass is releasedLOL! Yes I definitely did
Would you think it reasonable that the gains are relative to the persons ph experience? I often wonder about de-sensitization of the receptors as I do know for some people it seems to be chronic usage thus the need to megadose, whereas a person who rarely uses them e.g. 1 year + since the last run would benefit the most from the recommended dosage solo or in a stack?
I would stack both the 1dhea and 4dhea and having had 2 very short cycles (3 weeks approx) over 2 years ago, maybe the gains would be on the high end 8+?
Also when will alpha bulk be released?
They actually gave them 300mg's three times per day (t.i.d. = 3).I just read the study Pmid:21870106 and saw that the subjects consumed 300 mg's for 2 weeks afterwards the test was performed to evaluate the enzyme activity, and also noticed that there was a decrease in CYP2D6 between 0-8 h urinary dextromethorphan/dextrorphan increased ninefold.
Are they saying that the enzyme activity was already inhibited immediately after consuming 300 mg's of berberine as mentioned by 0-8h (0 - 8 hours after administration?).
I think I'll try to get around to posting a thread on Med Term in relationship to dosings and meds etc. Been meaning to do it for awhile now. Just see people posting off the wall abbv. for how many times a day and so forth and it always bugs me..lol. Not that it is bad or I get mad, but maybe it'll help people keep on the same track, just like in the medical community.They actually gave them 300mg's three times per day (t.i.d. = 3).
They gave them the drug(s) on day 1 before dosing any berberine and took blood and urine samples. Gave them berberine for two weeks, and on the last day gave them the same drug and took blood and urine sample. Then compared the two.
A lot if those terms are banned in hospitals now. We had a meeting a couple years back on why they are Jo longer allowed in our hospital.I think I'll try to get around to posting a thread on Med Term in relationship to dosings and meds etc. Been meaning to do it for awhile now. Just see people posting off the wall abbv. for how many times a day and so forth and it always bugs me..lol. Not that it is bad or I get mad, but maybe it'll help people keep on the same track, just like in the medical community.
i.g. B.I.D; T.I.D, Q.I.D; Q.D; I.M; S.Q, etc
Things like abbv for morphine are mso4 and such. Because of how similar they are to other notes, but much and most are still good. When I do it up, I'll do it based off of Joint Commision... THE standard which all hospitals are subjected to.A lot if those terms are banned in hospitals now. We had a meeting a couple years back on why they are Jo longer allowed in our hospital.
However the thread would be useful for those reading PubMed. Should make a "Deciphering Pub Med: For Dummies!" article!

like our new hats..figures they tossed me in for question on me assWe are doing a contest on our facebook page for free hats: http://www.facebook.com/pages/ForeRunner-Labs/130287063730239
They will not suggest this. Their hormone shield to my knowledge does not interact well with PP's. They have different opinions on the use of DHB and its effects on enzymes.With all that being said, I guess stacking this with PP's AM or AH would not be a good thing, or could it be? Or maybe I can stack with one or the other rather than both. If one or the other, which one?
^^^ This, PP's is less selective than FR, which I believe decreases down-stream conversion to the more favored metabolites. It'd be like using a scalpal and a chainsaw in the same incision of a surgery...They will not suggest this. Their hormone shield to my knowledge does not interact well with PP's. They have different opinions on the use of DHB and its effects on enzymes.
Is that what the V3.0 is all about?Plus if you wait, they will have PP equivalents out soon. They just need to get their line out.
I was talking about FRL's versions of PPs stuff. But V3.0 of Primordials are supposed to be better, higher doses and some ingredient changes. Plus the introduction of Androbulk which people believe to be a 19nor DHEAIs that what the V3.0 is all about?
Cant' wait for your loghat = sexy... so much want
can't wait til my precious bottles get to me
Truth? AH equivalent?Plus if you wait, they will have PP equivalents out soon. They just need to get their line out.
Don't think they have an Epiandrosterone product in the pipeline yet. I could be wrong though.Truth? AH equivalent?
Good question. Haven't seen any. Reps???Do we have any logs or reviews of forge runner products on here
Sorry can't advance search on a phone .. So if u suggest that .. Phhhhhhhhuuuuuuuck ju